Enter your email address
Submit

![]()
![]()
![]()


 , Hamed Aghaei2 , Taleb Askaripoor *3 , Mehdi Khazaei4 , Ehsan Bayat Khalaji4 , Elahe Kazemi4
, Hamed Aghaei2 , Taleb Askaripoor *3 , Mehdi Khazaei4 , Ehsan Bayat Khalaji4 , Elahe Kazemi4
Cranes, especially tower cranes, overhead cranes, gate cranes, and mobile cranes are recognized as critical equipment items in construction projects [1-3]. Despite the central role of cranes in construction operations, occupational fatalities and injuries resulting from their process have become a severe public problem [4, 5]. Some evidence has shown that cranes have been associated with more than one-third of all construction and maintenance process accidents [6-8]. Furthermore, tower cranes played a direct role in about 16% of these accidents [9]. Due to the size and power of cranes used in construction projects, the occurrence of accidents in these projects and threatening workers' safety and health can also cause injuries to people outside the project, such as pedestrians [6].
In recent years, increasing the cranes' technical quality has caused variables such as crane instability, jib instability, and hoisting equipment instability to play a lesser role in crane-related accidents [10]. On the other hand, according to the Labor Statistics Office [1, 2], 51% of accidents in construction projects were due to unknown causes. Besides, crane operators perform various highly repetitive tasks in one shift, including continuous monitoring of the transportation process, loading, unloading building materials, moving heavy steel plates, and adjusting final performance using unique control levers. Also, activity for the whole work shift (about 6 to 8 hours) in the cabin's limited space and their exposure to environmental conditions such as heat, cold, and radiance can impose a lot of mental load and stress on these employees [11, 12].
Based on the available evidence, if a product is designed to meet the needs of a particular group of users, product designers should use information specific to that group, including human factors and anthropometric dimensions [17]. The result of this process, while increasing the comfort and maintaining the health of employees, can reduce errors and improve safety. However, since crane cabins' design is mainly related to the 1960s; therefore, less attention has been paid to human factors and anthropometric dimensions in their structure [11]. Also, the minimal investigation has been done so far to evaluate the comfort and suitability of cabins with operators [18]. Due to the lack of studies in Iran to study cabin cranes' design from an ergonomic point of view, this study was conducted to assess the ergonomic risk of tower crane operators and redesign the dimensions and interior of the crane's cabin based on the anthropometric measurements of Iranian operators.
This study is a cross-sectional descriptive case study that was conducted in 2019. In this research, all tower crane operators working in three large construction projects in Tehran that met the inclusion criteria were studied. In this study, 30 operators (male; mean ± SD age; 37.8 ± 5.8 years) participated. Inclusion criteria included having at least one year of work experience and full-time employment as tower crane operators and not suffering from musculoskeletal disorders before starting work in this job. Exclusion criteria included unwillingness to participate in the study. After explaining the research objectives to all participants, they signed an informed consent form before starting the research. Also, the study protocol was approved (Ethics code; IR.SEMUMS.REC.1398.227) by the University Ethics Committee. In this investigation, a multi-stage approach was used to identify and define the problem and provide corrective solutions. First, to recognize and determine the problem accurately were used observational methods (view of physical condition and working conditions), interview (interview with operators and relevant officials to collect information about working conditions and physical condition and review of documents), Nordic questionnaire, and posture evaluation method (Rapid Upper Limb Assessment- RULA). Then, the studied operators' anthropometric data, machine design standards, and modeling were used to redesign tower crane cabin and interior dimensions. The steps of the study and its methodology are as follows (Figure 1):
| Check the existing situation |
| Observing, interviewing, and reviewing documents, assessing postures using the Rapid Upper Limb Assessment (RULA) method and evaluating the prevalence of musculoskeletal disorders using the Persian version of the Nordic Questionnaire |
| Select method and data collection for design |
|
| Final design |
| Complete and prepare the proposed cabin models |
Figure 1. Method study procedure
Step 1: Check the current situation
Field observation of working conditions, interviews with all operators and relevant officials, and review of documents were used to obtain an accurate image of the current situation, identify critical points, and determine the need for corrective interventions. The crane operators' working condition was evaluated using the RULA method (rapid upper limb assessment). Then, the prevalence of musculoskeletal disorders was assessed using the Persian version of the Nordic questionnaire. RULA (rapid upper limb assessment) is a survey method developed in 1993 for postures evaluation. In this method, the posture of the upper limbs of the body is evaluated using numerical scoring. The validity and reliability of this questionnaire have been proved in earlier studies [25-27]. An example of a tower crane cabin investigated in the present study is shown in Figure 2.

Figure 2. Existing tower crane cabin
Step 2: Determination and collection of the anthropometric dimensions of the study population
In this study, the relevant anthropometric dimensions for designing the crane cabin's dimensions and interior space were determined using previous research in tower crane design, existing standards, and guidelines for ergonomic design, and instructions for using anthropometric measurements in machine design. Anthropometric dimensions were measured in the usual coverage mode of operators, including work clothes and shoes. In this study, dimensions such as leg length, buttock-popliteal length, buttock width, arm length, shoulder width, forearm length, popliteal height, elbow height in sitting position, distance from elbow to elbow, eye height in sitting position were measured [3, 7, 18, 28-30].
Step 3: Redesign of tower crane cabin based on anthropometric dimensions of the studied operators
To redesign the tower crane cabin, machine design standards, instructions for using anthropometric dimensions in machine design [29, 32, 33], and previous studies in crane cabin design were used [3, 7, 18]. In this study, the length, width, and height of the cabin, the cabin entrance dimensions, the operator's seat, elbow rest, footrest, length, width, and size of the control panel were redesigned. Finally, Blender 2.82 3D modeling software was used to simulate the design. Data were analyzed using SPSS software version 20 (SPSS Inc., Chicago, Ill., USA) and descriptive statistics.
RULA's results in investigating the main tasks of tower crane operators showed that ergonomic intervention was necessary (Table 1).
| Left limbs | Right limbs | Type of Activity | ||
| Risk level | RULA final score | Risk level | RULA final score | |
| High | 6 | High | 6 | Load movement in the range of 360 degrees |
| High | 5 | High | 5 | Moving the load in the height range of the cabin and with a distance of more than 4 meters from the section |
| Very high | 7 | Very high | 7 | Moving the load in the area under the cabin and at a distance of fewer than 4 meters from the section |
Table 2. Frequency distribution of prevalence of musculoskeletal disorders based on the Nordic Musculoskeletal Questionnaire (NMQ)
| Frequency (%) | Area of body affected |
||
| Inability to work and activity due to pain and discomfort in the last 12 months | Had any musculoskeletal trouble in the last 7 days | Had any musculoskeletal trouble in the last 12 months | |
| - | 23.1 | Neck | |
| - | - | 7.7 | Shoulder |
| - | - | 7.7 | Forearm |
| - | 7.7 | 15.4 | Hands and wrists |
| - | 7.7 | 38.5 | Back |
| 7.7 | 15.4 | 61.5 | Low Back |
| 23.1 | - | - | One or both thighs |
| 15.4 | 38.5 | One or both knees | |
| 7.7 | - | - | One or both feet or ankles |
In this study, to design a crane cabin, Iranian operators' anthropometric dimensions related to design were collected. Mean, standard deviation, and percentiles 5 and 95 of these dimensions are presented in Table 3. Then, based on these dimensions, space's dimensions inside the room and the equipment inside it were redesigned. The redesign results for the interior tower crane cabin space are shown in Table 4 and Figure 3. Also, the inner cabin dimensions and the overall view of the cabin designed based on the output of the Blender 3D modeling software are shown in Figure 4.
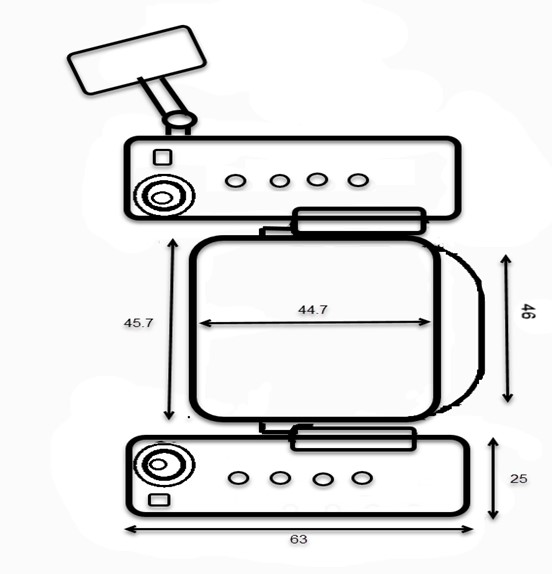
Figure 3. Dimensions of the redesign of room interior equipment

Figure 4. Overview and dimensions of the redesigned tower crane cabin
| Component | The obtained value (cm) |
| Operator seat height ( from cabin floor) | 40.7 to 47.3 |
| seat width | 45.7 |
| seat length | 44.7 |
| backrest width | 46 |
| Backrest height | 66.1 |
| Seat Slope | 0 ° to 10 ° |
| backrest angle | 3 ° to 7 ° |
| Headrest height | 23.1 to 31.7 |
| Headrest width | 27.2 |
| Elbow support height up to the seat level | 24.5 to 27.1 |
| Elbow support length | 20 |
| Between the two elbows supports distance | 47.9 |
| Elbow support width | 9.2 |
| Control panel height (from cabin floor ) | 65.2 to 74.4 |
| Control panel width | 25 |
| Control panel length | 63 |
| Pedaling space required | 87.5 |
| Elbow-fingertip length | 37.5 |
| Shoulder to fingertip length | 67.3 |
This study was conducted to assess the ergonomic risk of tower crane operator's activity and redesign the dimensions and interior space of the cabin of these cranes based on Iranian operators' anthropometric measurements in three large construction projects in Tehran. RULA's evaluation of working postures showed that the activities of tower crane operators were at a high and very high level of risk, which indicates the need for ergonomic intervention. Since so far, no study in Iran has investigated tower crane operators' working postures, it is impossible to compare the present study results with other studies. The study by Veljković et al. showed that most of the working postures and interior design of the crane cabin studied in Serbia were at an unacceptable level, which is consistent with the results of the present study [34].
The investigation results indicated that 85% of the studied operators in the past 12 months reported pain and discomfort in one area of the body, including the neck, shoulders, back, forearms, hands and wrists, thighs, knees, and legs. Moreover, the highest pain prevalence was related to low back with 61.5%, followed by knees and back with 38.5%. Consistent with these findings, Kushwaha and Kane reported that almost all crane operators in the Indian steel industry had been consistently experiencing a type of musculoskeletal disorder for the past year [11].
Based on the present study's results on the evaluation of working postures by the RULA and the prevalence of musculoskeletal disorders and other studies' findings, the problem's root can be due to human factors engineering disregard and improper design of the crane cabin. Given that human factor engineering (ergonomics) is the science of studying human-machine interaction in the workplace to improve worker performance and reduce stress and fatigue [11]. Therefore, ergonomic interventions such as redesigning the operator workstation based on the target population's anthropometric dimensions and not the general population and reconsidering crane operators' tasks seem necessary [31]. The result of this process can prevent work-related injuries and fatality, improve safety and productivity.
In this study, based on Iranian operators' anthropometric dimensions, the tower crane cabin's dimensions were redesigned. Accordingly, the dimensions of the redesigned cabin were 160.8 × 144.1 × 199.7 cm, which is slightly different from the sizes recommended by the standard ISO 8566-5 (160 × 130 × 200 cm) [33]. Also, in the mentioned studies and ISO 8566-5, the study population is women and men, and anthropometric dimensions of women have been used to determine the cabin's measurements. However, in the present study, due to Iran's cultural differences and the lack of employment of women as crane operators, only the anthropometric dimensions of men were used, which can also explain the difference between the obtained sizes and other studies. The cabins' height in the project's understudy in the present study was 237 and 190 cm, which needs to be reconsidered in cabins with a height lower than the value obtained in the present study (199.7 cm). Although the other dimensions of existing cabins, such as the cabin's length and width and the height and width of the cabin's entrance door, are larger than the values obtained in the current study, no problem is observed in this regard.
According to the study results from the perspective of ergonomic risk assessment, the activities of tower crane operators were at a high level of risk, and the prevalence of musculoskeletal disorders was high among them. Hence, crane cabins' interior design does not meet the operator's needs. The use of corrective and redesign interventions to increase human-machine compatibility, improve safety, and prevent musculoskeletal injuries seems essential.
The author would like to acknowledge the University Student Research Committee, construction project managers, and all participants for their invaluable support during this project.
The authors declared no conflict of interest.
Authors of the manuscript have not received any funding for the present study.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |